
Recovery from gaming addiction: A thematic synthesis
Vol.18,No.2(2024)
Alex Kyriakopoulos
 Christopher Wilson
Christopher Wilson
In recent years the field of gaming addiction has experienced an upsurge in empirical studies on various treatment approaches. Despite the advances in our understanding of how gaming addiction can be treated, the wider concept of recovery continues to be under-researched. The purpose of this review was to explore how individuals addicted to video games experience the process of recovery. Seven databases were systematically searched for qualitative studies. Eight studies representing the views of 225 participants were included in the review. Study findings were exported into NVivo software and analysed using Thematic Synthesis. Six themes were constructed: “developing awareness”, “deciding to change”, “the process of quitting”, “the challenges of quitting”, “recovery never stops” and “treatment for gaming addiction”. Except for the last, themes represent processes that most participants had gone through during recovery, though significant variation was found in how each process was experienced. In addition to overcoming addiction symptoms, recovery involved management of concomitant problems and various negative consequences of excessive gaming. Regarding practice implications, current findings suggest that treatment programs should adopt a multidimensional approach, providing evidence-based treatments, help for co-occurring problems, as well as pre- and post-treatment support to accommodate individuals at different stages of recovery. Further research is needed to expand our understanding of recovery, for instance, the impact of gender differences or how recovery experiences change based on different recovery goals (i.e., abstinence or reduced play time).
gaming disorder; addiction; thematic synthesis; recovery; rapid review
Ksenija Vasiljeva
Department of Psychology, Teesside University
Ksenija Vasiljeva is a doctoral student on the program of Doctorate in Counselling Psychology at Teesside University. Her research interests include gaming addiction, depressive disorders, and cultural studies.
Alex Kyriakopoulos
Department of Psychology, Teesside University
Alexandros Kyriakopoulos is a Senior Lecturer in Counselling Psychology at Teesside University. He is interested in research regarding applied cyberpsychology; e-parenting; e-wellbeing; and using e-interventions to improve mental health and wellbeing.
Christopher Wilson
Department of Psychology, School of Social Sciences, Humanities and Law, Teesside University, Middlesbrough, United Kingdom
Christopher Wilson is currently an Associate Professor in Psychology at Teesside University. He obtained his PhD from Maynooth University in 2010 where he was awarded a scholarship for doctoral research by the Irish Research Council (IRCHSS). His research interests include: Risk-taking and decision-making; attention and perception; Behaviour and cognition in virtual and online environments.
Studies marked with an (*) were included in the review.
*Beranuy, M., Carbonell, X., & Griffiths, M. D. (2013). A qualitative analysis of online gaming addicts in treatment. International Journal of Mental Health and Addiction, 11(2), 149–161. https://doi.org/10.1007/s11469-012-9405-2
Best, D. W., & Lubman, D. I. (2012). The recovery paradigm: A model of hope and change for alcohol and drug addiction. Australian Family Physician, 41(8), 593–597. https://pubmed.ncbi.nlm.nih.gov/23145400/
*Carmona, J., & Whiting, J. B. (2021). Escaping the escapism: A grounded theory of the addiction and recovery process in online video gaming. Qualitative Report, 26(7), 2171–2188. https://doi.org/10.46743/2160-3715/2021.4643
*Chappell, D., Eatough, V., Davies, M. N. O., & Griffiths, M. (2006). EverQuest - It’s just a computer game right? An interpretative phenomenological analysis of online gaming addiction. International Journal of Mental Health and Addiction, 4(3), 205–216. https://doi.org/10.1007/s11469-006-9028-6
Cooke, A., Smith, D., & Booth, A. (2012). Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qualitative Health Research, 22(10), 1435–1443. https://doi.org/10.1177/1049732312452938
Costello, M. J., Sousa, S., Ropp, C., & Rush, B. (2020). How to measure addiction recovery? Incorporating perspectives of individuals with lived experience. International Journal of Mental Health and Addiction, 18(3), 599–612. https://doi.org/10.1007/s11469-018-9956-y
Coyne, S. M., Stockdale, L. A., Warburton, W., Gentile, D. A., Yang, C., & Merrill, B. M. (2020). Pathological video game symptoms from adolescence to emerging adulthood: A 6-year longitudinal study of trajectories, predictors, and outcomes. Developmental Psychology, 56(7), 1385–1396. https://doi.org/10.1037/dev0000939
Critical Appraisal Skills Programme. (2018). CASP qualitative checklist. https://casp-uk.net/casp-tools-checklists/
Dekkers, A., Bellaert, L., Meulewaeter, F., De Ruysscher, C., & Vanderplasschen, W. (2021). Exploring essential components of addiction recovery: A qualitative study across assisted and unassisted recovery pathways. Drugs: Education, Prevention, and Policy, 28(5), 486–495. https://doi.org/10.1080/09687637.2021.1943315
Dong, G.-H., & Potenza, M. N. (2022). Considering gender differences in the study and treatment of Internet gaming disorder. Journal of Psychiatric Research, 153, 25–29. https://doi.org/10.1016/j.jpsychires.2022.06.057
el-Guebaly, N. (2012). The meanings of recovery from addiction: Evolution and promises. Journal of Addiction Medicine, 6(1), 1–9. https://doi.org/10.1097/ADM.0b013e31823ae540
Entertainment Software Association. (2023). 2023 essential facts about the U.S. video games industry. https://www.theesa.com/2023-essential-facts/
Ferreira, A. C. Z., Capistrano, F. C., Souza, E. B., Borba, L. O., Kalinke, L. P., & Maftum, M. A. (2015). Drug addicts treatment motivations: Perception of family members. Revista Brasileira de Enfermagem, 68(3), 415–422. https://doi.org/10.1590/0034-7167.2015680314i
Gandolfi, E., Ferdig, R. E., Krause, K., Soyturk, I., Morris, G., & Delahanty, S. (2023). An exploration of why gaming communities may make younger and non-normative gamers vulnerable to Internet gaming disorder. New Media & Society. Advance online publication. https://doi.org/10.1177/14614448231215348
Gavriel-Fried, B., Serry, M., Katz, D., Hidvégi, D., Demetrovics, Z., & Király, O. (2023). The concept of recovery in gaming disorder: A scoping review. Journal of Behavioral Addictions, 12(1), 26–52. https://doi.org/10.1556/2006.2023.00002
Goshorn, J. R., Gutierrez, D., & Dorais, S. (2023). Sustaining recovery: What does it take to remain in long-term recovery? Substance Use & Misuse, 58(7), 900–910. https://doi.org/10.1080/10826084.2023.2196557
Goslar, M., Leibetseder, M., Muench, H. M., Hofmann, S. G., & Laireiter, A. (2020). Treatments for Internet addiction, sex addiction and compulsive buying: A meta-analysis. Journal of Behavioral Addictions, 9(1), 14–43. https://doi.org/10.1556/2006.2020.00005
Grall-Bronnec, M., Guillou-Landreat, M., Caillon, J., Dubertret, C., Romo, L., Codina, I., Chereau-Boudet, I., Lanson, C., Auriacombe, M., JEU-Group, Harduin, J. B., & Reynaud, M. (2021). Five-year follow-up on a sample of gamblers: Predictive factors of relapse. Journal of Behavioral Addictions, 10(1), 42–54. https://doi.org/10.1556/2006.2021.00009
*Haagsma, M. C., Pieterse, M. E., Peters, O., & King, D. L. (2013). How gaming may become a problem: A qualitative analysis of the role of gaming related experiences and cognitions in the development of problematic game behavior. International Journal of Mental Health and Addiction, 11(4), 441–452. https://doi.org/10.1007/s11469-013-9427-4
Hofstedt, A., Mide, M., Arvidson, E., Ljung, S., Mattiasson, J., Lindskog, A., & Soderpalm-Gordh, A. (2023). Pilot data findings from the Gothenburg treatment for gaming disorder: A cognitive behavioral treatment manual. Frontiers in Psychiatry, 14, Article 1162492. https://doi.org/10.3389/fpsyt.2023.1162492
James, R. J. E., & Tunney, R. J. (2017). The need for a behavioural analysis of behavioural addictions. Clinical Psychology Review, 52, 69–76. https://doi.org/10.1016/j.cpr.2016.11.010
*Karhulahti, V.-M., Siutila, M., Vahlo, J., & Koskimaa, R. (2022). Phenomenological strands for gaming disorder and esports play: A qualitative registered report. Collabra: Psychology, 8(1), Article 38819. https://doi.org/10.1525/collabra.38819
Kelly, J. F., & White, W. L. (2011). Recovery management and the future of addiction treatment and recovery in the USA. In J. F. Kelly & W. L. White (Eds.), Addiction recovery management: Theory, research and practice (pp. 303–316). Humana Press. https://psycnet.apa.org/record/2010-25515-016
Kim, H. S., Son, G., Roh, E.-B., Ahn, W.-Y., Kim, J., Shin, S.-H., Chey, J., & Choi, K.-H. (2022). Prevalence of gaming disorder: A meta-analysis. Addictive Behaviors, 126, Article 107183. https://doi.org/10.1016/j.addbeh.2021.107183
Kim, J., Lee, S., Lee, D., Shim, S., Balva, D., Choi, K. H., Chey, J., Shin, S. H., & Ahn, W. Y. (2022). Psychological treatments for excessive gaming: A systematic review and meta-analysis. Scientific Reports, 12(1), Article 20485. https://doi.org/10.1038/s41598-022-24523-9
King, D. L., & Delfabbro, P. H. (2018). Internet gaming disorder: Theory, assessment, treatment, and prevention. Elsevier Academic Press. https://psycnet.apa.org/record/2018-35840-000
Kotyuk, E., Magi, A., Eisinger, A., Király, O., Vereczkei, A., Barta, C., Griffiths, M. D., Székely, A., Kökönyei, G., Farkas, J., Kun, B., Badgaiyan, R. D., Urbán, R., Blum, K., & Demetrovics, Z. (2020). Co-occurrences of substance use and other potentially addictive behaviors: Epidemiological results from the psychological and genetic factors of the addictive behaviors (PGA) study. Journal of Behavioral Addictions, 9(2), 272–288. https://doi.org/10.1556/2006.2020.00033
Kougiali, Z. G., Fasulo, A., Needs, A., & Van Laar, D. (2017). Planting the seeds of change: Directionality in the narrative construction of recovery from addiction. Psychology & Health, 32(6), 639–664. https://doi.org/10.1080/08870446.2017.1293053
Kushnir, V., Godinho, A., Hodgins, D. C., Hendershot, C. S., & Cunningham, J. A. (2016). Motivation to quit or reduce gambling: Associations between self-determination theory and the transtheoretical model of change. Journal of Addictive Diseases, 35(1), 58–65. https://doi.org/10.1080/10550887.2016.1107315
Laier, C., & Brand, M. (2014). Empirical evidence and theoretical considerations on factors contributing to cybersex addiction from a cognitive-behavioral view. Sexual Addiction & Compulsivity, 21(4), 305–321. https://doi.org/10.1080/10720162.2014.970722
Leamy, M., Bird, V., Boutillier, C. L., Williams, J., & Slade, M. (2011). Conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. The British Journal of Psychiatry, 199(6), 445–452. https://doi.org/10.1192/bjp.bp.110.083733
Lucas, P. J., Baird, J., Arai, L., Law, C., & Roberts, H. M. (2007). Worked examples of alternative methods for the synthesis of qualitative and quantitative research in systematic reviews. BMC Medical Research Methodology, 7, Article 4. https://doi.org/10.1186/1471-2288-7-4
Männikkö, N., Ruotsalainen, H., Miettunen, J., Pontes, H. M., & Kääriäinen, M. (2020). Problematic gaming behaviour and health-related outcomes: A systematic review and meta-analysis. Journal of Health Psychology, 25(1), 67–81. https://doi.org/10.1177/1359105317740414
Marraudino, M., Bonaldo, B., Vitiello, B., Bergui, G. C., & Panzica, G. (2022). Sexual differences in Internet gaming disorder (IGD): From psychological features to neuroanatomical networks. Journal of Clinical Medicine, 11(4), Article 1018. https://doi.org/10.3390/jcm11041018
Martinelli, T. F., Roeg, D. P. K., Bellaert, L., Van de Mheen, D., & Nagelhout, G. E. (2023). Understanding the process of drug addiction recovery through first-hand experiences: A qualitative study in the Netherlands using lifeline interviews. Qualitative Health Research, 33(10), 857–870. https://doi.org/10.1177/10497323231174161
Mihara, S., & Higuchi, S. (2017). Cross-sectional and longitudinal epidemiological studies of Internet gaming disorder: A systematic review of the literature. Psychiatry and Clinical Neurosciences, 71(7), 425–444. https://doi.org/10.1111/pcn.12532
Müller, K. W., Wolfling, K., Dickenhorst, U., Beutel, M. E., Medenwaldt, J., & Koch, A. (2017). Recovery, relapse, or else? Treatment outcomes in gambling disorder from a multicenter follow-up study. European Psychiatry, 43, 28–34. https://doi.org/10.1016/j.eurpsy.2017.01.326
Nakayama, H., Matsuzaki, T., Mihara, S., Kitayuguchi, T., & Higuchi, S. (2020). Relationship between problematic gaming and age at the onset of habitual gaming. Pediatrics International, 62(11), 1275–1281. https://doi.org/10.1111/ped.14290
Neale, J., Tompkins, C., Wheeler, C., Finch, E., Marsden, J., Mitcheson, L., Rose, D., Wykes, T., & Strang, J. (2015). “You’re all going to hate the word ‘recovery’ by the end of this”: Service users’ views of measuring addiction recovery. Drugs: Education, Prevention and Policy, 22(1), 26–34. https://doi.org/10.3109/09687637.2014.947564
Newzoo. (2023). Global games market report. https://newzoo.com/resources/trend-reports/newzoo-global-games-market-report-2023-free-version
Nilsson, A., Simonsson, O., & Hellner, C. (2023). Reasons for dropping out of Internet-based problem gambling treatment, and the process of recovery – A qualitative assessment. Current Psychology, 42, 10987–10998. https://doi.org/10.1007/s12144-021-02368-1
Oakes, J., Pols, R., & Lawn, S. (2019). The ‘merry-go-round’ of habitual relapse: A qualitative study of relapse in electronic gaming machine problem gambling. International Journal of Environmental Research and Public Health, 16(16), Article 2858. https://doi.org/10.3390/ijerph16162858
Ofcom. (2023). Online nation: 2023 report. https://www.ofcom.org.uk/research-and-data/online-research/online-nation
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., Shamseer, L., Tetzlaff, J. M., Akl, E. A., Brennan, S. E., Chou, R., Glanville, J., Grimshaw, J. M., Hróbjartsson, A., Lalu, M. M., Li, T., Loder, E. W., Mayo-Wilson, E., McDonald, S., … & Moher, D. (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ, 372, Article n71. https://doi.org/10.1136/bmj.n71
*Park, J. J., Wilkinson-Meyers, L., King, D. L., & Rodda, S. N. (2021). Person-centred interventions for problem gaming: A stepped care approach. BMC Public Health, 21, Article 872. https://doi.org/10.1186/s12889-021-10749-1
Pickering, D., Spoelma, M. J., Dawczyk, A., Gainsbury, S. M., & Blaszczynski, A. (2020). What does it mean to recover from a gambling disorder? Perspectives of gambling help service users. Addiction Research and Theory, 28(2), 132–143. https://doi.org/10.1080/16066359.2019.1601178
Prochaska, J. O., & DiClemente, C. C. (2005). The transtheoretical approach. In J. C. Norcross & M. R. Goldfried (Eds.), Handbook of psychotherapy integration (2nd ed., pp. 147–171). Oxford University Press. https://doi.org/10.1093/med:psych/9780195165791.003.0007
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictive behaviors. The American Psychologist, 47(9), 1102–1114. https://doi.org/10.1037//0003-066x.47.9.1102
Reith, G., & Dobbie, F. (2012). Lost in the game: Narratives of addiction and identity in recovery from problem gambling. Addiction Research and Theory, 20(6), 511–521. https://doi.org/10.3109/16066359.2012.672599
Scott, C. K., & Dennis, M. L. (2011). Recovery management checkups with adult chronic substance users. In J. F. Kelly & W. L. White (Eds.), Addiction recovery management: Theory, research and practice (pp. 87–101). Humana Press. https://psycnet.apa.org/record/2010-25515-006
Sherer, J., & Levounis, P. (2022). Technological addictions. Current Psychiatry Report, 24, 399–406. https://doi.org/10.1007/s11920-022-01351-2
*Sim, T., Choo, H., Low-Lim, A., & Lau, J. (2021). Adolescents’ and parents’ perspectives: A gaming disorder intervention in Singapore. Family Relations, 70(1), 90–103. https://doi.org/10.1111/fare.12474
Sirola, A., Savela, N., Savolainen, I., Kaakinen, M., & Oksanen, A. (2021). The role of virtual communities in gambling and gaming behaviors: A systematic review. Journal of Gambling Studies, 37, 165–187. https://doi.org/10.1007/s10899-020-09946-1
Snodgrass, J. G., Dengah, H. J. F. 2nd, Lacy, M. G., & Fagan, J. (2013). A formal anthropological view of motivation models of problematic MMO play: Achievement, social, and immersion factors in the context of culture. Transcultural Psychiatry, 50(2), 235–262. https://doi.org/10.1177/1363461513487666
Stefani, C. (2023). Determinants of initiation of natural recovery in the case of slot machine abusers. Journal of Community Positive Practices, 1, 84–95. https://doi.org/10.35782/JCPP.2023.1.07
Stevens, M. W. R., Dorstyn, D., Delfabbro, P. H., & King, D. L. (2021). Global prevalence of gaming disorder: A systematic review and meta-analysis. Australian and New Zealand Journal of Psychiatry, 55(6), 553–568. https://doi.org/10.1177/0004867420962851
Stevens, M. W. R., King, D. L., Dorstyn, D., & Delfabbro, P. H. (2019). Cognitive-behavioral therapy for Internet gaming disorder. A systematic review and meta-analysis. Clinical Psychology & Psychotherapy, 26(2), 191–203. https://doi.org/10.1002/cpp.2341
Sugaya, N., Shirasaka, T., Takahashi, K., & Kanda, H. (2019). Bio-psychosocial factors of children and adolescents with Internet gaming disorder: A systematic review. BioPsychoSocial Medicine, 13, Article 3. https://doi.org/10.1186/s13030-019-0144-5
Sun, Y., & Zhang, Y. (2021). A review of theories and models applied in studies of social media addiction and implications for future research. Addictive Behaviors, 114, Article 106699. https://doi.org/10.1016/j.addbeh.2020.106699
Sussman, S. Y., Ayala, N., & Pokhrel, P. (2022). Reflections on the continued popularity of the transtheoretical model. Health Behavior Research, 5(3), Article 2. https://doi.org/10.4148/2572-1836.1128
Thomas, J., & Harden, A. (2008). Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Medical Research Methodology, 8, Article 45. https://doi.org/10.1186/1471-2288-8-45
Tseng, M.-F., Huang, C.-C., Tsai, S. C.-S., Tsay, M.-D., Chang, Y.-K., Juan, C.-L., Hsu, F.-C., & Wong, R.-H. (2022). Promotion of smoking cessation using the transtheoretical model: Short-term and long-term effectiveness for workers in coastal central Taiwan. Tobacco Use Insights, 15, 1–10. https://doi.org/10.1177/1179173x221104410
Watkins, N., Brown, A. M., & Courson, K. (2021). Identity transformation through substance use disorder recovery: Introducing the six stage model. Qualitative Report, 26(7), 2127–2151. https://doi.org/10.46743/2160-3715/2021.4918
*Wendt, L. M., Austermann, M. I., Rumpf, H. J., Thomasius, R., & Paschke, K. (2021). Requirements of a group intervention for adolescents with Internet gaming disorder in a clinical setting: A qualitative interview study. International Journal of Environmental Research and Public Health, 18(15), Article 7813. https://doi.org/10.3390/ijerph18157813
White, W. L. (2007). Addiction recovery: Its definition and conceptual boundaries. Journal of Substance Abuse Treatment, 33(3), 229–241. https://doi.org/10.1016/j.jsat.2007.04.015
White, W. L., & Kelly, J. F. (2011). Recovery management: What if we really believed that addiction was a chronic disorder? In J. F. Kelly & W. L. White (Eds.), Addiction recovery management: Theory, research and practice (pp. 67–84). Humana Press. https://psycnet.apa.org/record/2010-25515-005
Witkiewitz, K., Montes, K. S., Schwebel, F. J., & Tucker, J. A. (2020). What is recovery? Alcohol Research: Current Reviews, 40(3), Article 1. https://doi.org/10.35946/arcr.v40.3.01
World Health Organisation. (2018, September 14). Inclusion of “gaming disorder” in ICD-11. https://www.who.int/news/item/14-09-2018-inclusion-of-gaming-disorder-in-icd-11#:~:text=Gaming%20disorder%2C%20with%20its%20online%20and%20offline%20variants%2C,in%20personal%2C%20family%2C%20social%2C%20educational%20or%20occupational%20functioning.
World Health Organization. (2023). ICD-11: International classification of diseases (11th revision). https://icd.who.int/
Xiao, Y., & Watson, M. (2019). Guidance on conducting a systematic literature review. Journal of Planning Education and Research, 39(1), 93–112. https://doi.org/10.1177/0739456X17723971
Yates, R., & Malloch, M. S. (2010). The road less travelled? A short history of addiction recovery. In R. Yates, & M. S. Malloch (Eds.), Tackling addiction: Pathways to recovery (pp. 15–31). Jessica Kingsley Publishers.
Authors’ Contribution
Ksenija Vasiljeva: conceptualization, methodology, investigation, formal analysis, writing—original draft. Alexandros Kyriakopoulos: conceptualization, writing—review & editing, supervision. Christopher Wilson: supervision.
Editorial Record
First submission received:
October 19, 2023
Revisions received:
March 3, 2024
Accepted for publication:
March 11, 2024
Editor in charge:
Lenka Dedkova
Introduction
According to Newzoo report, there were 3.38 billion video game players globally in 2023, and this number is forecast to rise to 3.79 billion by 2026 (Newzoo, 2023). In the UK, 56% of adults and 91% of children play video games (Ofcom, 2023). Similarly, the statistics for the US are 62% and 76% respectively (Entertainment Software Association, 2023). Although gaming is an important recreational activity for many people, some individuals may play excessively to the detriment of their health, wellbeing, interpersonal relationships, and occupational opportunities (Mihara & Higuchi, 2017; Sugaya et al., 2019). A longitudinal study by Coyne et al. (2020) found that participants who played games excessively had elevated levels of anxiety, depression, aggression, shyness, and cell phone use. Problematic gaming behaviour has been linked to adverse health outcomes, such as poorer sleep quality, reduced physical activity and hand and wrist pain (Männikkö et al., 2020). Socially, excessive gaming can result in deteriorating personal relationships, occupational problems, and overall worse quality of life (Carmona & Whiting, 2021).
Mounting evidence of the negative impact of excessive gaming led the World Health Organisation to include a diagnosis of “Gaming disorder” (GD) in the latest edition of International Classification of Diseases (ICD-11; WHO, 2018, 2023). According to ICD-11, three criteria must be met over a period of 12 months for a diagnosis of GD: impaired control over gaming behaviour (e.g., duration, termination), gaming is given priority over other life interests and activities, and gaming is continued or escalates despite the occurrence of negative consequences (WHO, 2023). Stevens and colleagues (2021) estimated that the global prevalence of GD is 3.05%, which was reduced to 1.96% when including studies that met strict sampling criteria. A meta-analysis by H. S. Kim et al. (2022) similarly found that the global prevalence of GD was 3.3%. Both studies found that young age and male gender were associated with higher prevalence.
Recovery is a “process of behavior change characterized by improvements in biopsychosocial functioning and purpose in life” (Witkiewitz et al., 2020, p. 9). It is a multidimensional and complex phenomenon. Leamy and colleagues (2011), for instance, argue that recovery consists of the following five dimensions: connectedness (relationships, community participation), hope and optimism about the future (motivation to change, aspirations), identity (rebuilding identity, overcoming stigma), meaning in life (spirituality, quality of life) and empowerment (personal responsibility, control over life). This theoretical conceptualisation is supported by the experiences of individuals in recovery. For instance, in Dekkers et al. (2021) study participants’ recovery encompassed developing a new sense of self, feeling supported by others, finding safe places of growth, and working towards a better future. In a study of participants in residential treatment, recovery was conceived as abstinence coupled with positive gains on at least one of the following psychosocial dimensions: psychological, physical health, spiritual, occupational, social relations, or daily life functioning (Costello et al., 2020).
Our evolving understanding of recovery has directly shaped the development of treatment approaches. Historically, addiction was conceptualised as a physical disease that deprived people of free will; hence, it was believed that recovery was only achievable through medical interventions (Yates & Malloch, 2010). Treatment often took the form of acute care (i.e., crisis support and inpatient treatment), a person was considered “cured” from addiction at the end of treatment (White & Kelly, 2011). Although the disease model is still prevalent, the emphasis has shifted to viewing addiction as a chronic condition (Best & Lubman, 2012). This re-conceptualisation brought with it the idea that addiction should be treated similarly to other chronic conditions by offering ongoing long-term support (Scott & Dennis, 2011). Recovery-oriented treatments focus on early detection and intervention, provision of community services, peer support groups and residential programs (Kelly & White, 2011). Although acute care is still used at crisis points, preference is given to administering treatment in the community and helping individuals achieve their personal recovery goals. This aligns with service users’ experience of recovery as a long-term process that is more about personal growth and psychosocial improvement than achieving a definitive “cure” (Costello et al., 2020; Neale et al., 2015; Pickering et al., 2020). Therefore, the way we treat addiction has changed as a result of re-conceptualising recovery as a chronic condition.
Within the field of gaming addiction, the notion of recovery is only starting to take shape. Gavriel-Fried et al. (2023) conducted a scoping review, investigating how GD treatment studies (n = 47) conceptualised recovery. Most studies (n = 42) used terms “decrease/reduction” and/or “increase/improvement” of symptoms to describe changes in participants’ GD before and after interventions. Although the term “recovery” was mentioned by 18 studies, only 5 of them discussed it in relation to study aims, hypotheses, sample characteristics or findings. These studies conceptualised recovery as reduction in GD scores and/or no longer meeting the criteria for a GD diagnosis. Despite the limited use of the term “recovery”, all 47 studies included at least one psychological (n = 32), neurobiological (n = 20) and/or social (n = 7) measure to evaluate the impact of treatment. It was found that certain personality traits (impulsivity, higher aggression, harm avoidance) and comorbid disorders (ADHD, depression) hinder patient recovery, whereas treatment (psychotherapy, medication) and social factors (family support) promote recovery. Although the review showed that the efficacy of GD treatments was evaluated against various psychosocial and neurobiological dimensions, there was no fundamental agreement on what “recovery” is beyond a person no longer meeting the diagnostic criteria for GD. Furthermore, only 13 studies in this review measured positive improvement (e.g., wellbeing, family cohesion, quality of life). This contrasts with the notions of recovery discussed earlier that advocate for focusing less on pathology and amelioration of disease in favour of helping individuals develop strength and resilience to live the life of greatest value to them (Witkiewitz et al., 2020).
Cognitive-Behavioural Therapy (CBT) is currently considered to be the gold standard of GD treatment (Stevens et al., 2019). Therapy covers topics such as stimulus control, cognitive restructuring, behavioural activation, relapse prevention and others (Hofstedt et al., 2023). Treatment usually lasts between 8 to 12 weeks, with follow up at 2 to 6 months (Stevens et al., 2019). Although CBT is an effective treatment, the way it is often delivered as a standalone intervention with no further support provided aligns more closely with the acute, rather than the chronic care provision pathway. J. Kim et al. (2022) evaluated different psychological interventions for GD and concluded that CBT+mindfulness, CBT+family therapy, and mindfulness were superior treatments to standalone CBT. Addiction recovery research emphasises that the best treatment outcomes are achieved when adopting a holistic approach that combines personal, relational, and contextual aspects (Dekkers et al., 2021) which may explain why combined treatments were more effective than standalone CBT in J. Kim et al. (2022) study.
It has been argued that Internet-based addictions (gaming, gambling, pornography, shopping, social media) share common aetiology, developing through behavioural conditioning, with predisposing neurobiological, individual and social factors (James & Turney, 2017; Kotyuk et al., 2020; Laier & Brand, 2014; Sun & Zhang, 2021). CBT for Internet Addiction (includes behaviour modification, cognitive restructuring, harm reduction) has been recommended as the treatment of choice for all Internet-based addictions, irrespective of the type (Goslar et al., 2020; Sherer & Levounis, 2022). However, even if Internet-based addictions develop through similar mechanisms, they are qualitatively and experientially different. Gaming is unique in that it offers highly rewarding, immersive and interactive environments, creating a more appealing reality than individuals’ day-to-day experiences (King & Delfabbro, 2018). Some individuals may use in-game achievements to compensate for their perceived offline “failures”, becoming overly invested in gaming to satisfy psychological needs (Snodgrass et al., 2013). Being part of an online gaming community is important for the development of gaming-related identity (Sirola et al., 2021). However, it was also shown that online communities play an important role in informing GD (Gandolfi et al., 2023), and community engagement can motivate escalation of gaming and in-game purchasing behaviours (Sirola et al., 2021). Furthermore, unlike many other addictive behaviours, gaming is accessible to very young children. Earlier onset of habitual weekly gaming (5 years old and younger) increases the risk of problematic gaming in adolescence (Nakayama et al., 2020). From these examples it can be seen that despite sharing aetiology with other addictions, there are key differences that may affect treatment prospects and recovery.
To reiterate, having a robust definition of recovery is fundamental for developing better treatments. However, at this point in time, there is no shared understanding of what recovery from GD looks like, and whether it is different to other Internet-based addictions. Our current conceptualisation of recovery is based on quantitative evidence which is limited to investigating changes in psychosocial and neurobiological symptoms (Gavriel-Fried et al., 2023). However, as discussed above, recovery may encompass processes not easily captured by psychometric measures, such as identity change, meaning in life and empowerment (Leamy et al., 2011). To the best of the author’s knowledge this is the first review sought to develop a conceptualisation of GD recovery by employing qualitative methodology to investigate the topic of recovery inductively, drawing on lived experiences of individuals affected by GD. The guiding review question was:
RQ1: How do individuals addicted to playing video games experience recovery?
Methods
Search Strategy
The literature review protocol was registered with PROSPERO. The review adopted a systematic search methodology in accordance with PRISMA guidelines (Page et al., 2021). The following databases were searched: PubMED, PsycINFO, PsycArticles, Scopus, Cinahl, Web of Science and MedLine. Search terms were chosen according to selection criteria using SPIDER framework (Cooke et al., 2012). Key terms included a combination of synonyms for “gaming”, “addiction”, “interview”, “experience” and “qualitative” (see Table A1 for a full list of terms). The searches were run on 1st November 2022. References were exported into Mendeley. Articles were sifted by title and abstract, articles that clearly did not meet the selection criteria were excluded. Full-text articles were retrieved for the remaining records and assessed for eligibility. Additional articles were identified through reference lists of included studies and Google Scholar. The search and sifting were carried out by the first author.
Selection Criteria
Studies were included if they represented original qualitative research and had information relevant to recovery from gaming addiction. Studies could use any method of data collection or analysis. Importantly, studies had to represent opinions, insights and experiences of people who are or have been addicted to video games. Sample could include individuals of any age and could be clinical (diagnosis of GD) or non-clinical (self-reported addiction to video games). Since this review was primarily interested in people’s experiences of gaming addiction, rather than homogeneity of results, a diagnosis of GD was not considered essential. No restrictions were set based on the year of publication. Only peer-reviewed articles in English were included. Studies were excluded, if they: 1. had quantitative design, 2. focused on individuals without gaming addiction (e.g., healthy gamers, parents and spouses of people with GD, health professionals), 3. had no information relevant to recovery from gaming addiction, 4. thesis or grey literature.
Data Extraction
Descriptive data was entered into an Excel spreadsheet. The following information was extracted: Title, Authors, Year, Country, Aims/Questions, Theoretical framework, Context, Method of recruitment, Participants (N; age: M, range; N: female), Method of data collection, Method of analysis, Notes. See Table A3 for the full data extraction table. To prepare qualitative data for analysis, findings of included studies were copied into separate Word documents and uploaded to Nvivo 12. In this study, “findings” were considered to be everything in the “Results” section, including text, tables, participant quotes and authors’ interpretations. However, since the review is interested in the recovery process from the perspective of individuals addicted to gaming, accounts of parents and health professionals were not included in the analysis, even if they were present in the “Results” section.
Data Analysis
Data was analysed using thematic synthesis (Thomas & Harden, 2008). During the planning stages of the review the first author scoped the literature to determine whether there was sufficient material for a review. The extent to which recovery was discussed differed greatly across studies. Some studies had a separate theme dedicated to it, while others mentioned it in passing, meaning that findings would need to be re-analysed to identify processes relevant to recovery. Therefore, chosen analytical strategy had to be interpretative, rather than descriptive or aggregative. Thematic synthesis is a flexible interpretative approach, suitable for drawing together common elements from heterogenous studies (Lucas et al., 2007). Furthermore, it aims to produce new, higher-order constructs that go beyond individual findings of primary studies (Xiao & Watson, 2019). Given that the aim of this review was to develop a conceptualisation of GD recovery, thematic synthesis was considered to be a suitable method of analysis.
Analysis was conducted in three stages: free line-by-line coding, organisation of free codes into descriptive themes and creation of analytical themes. Line-by-line coding is inductive analysis of each sentence to consider its meaning and content. This process ensures that all data is carefully considered, even if not all sentences get coded (Thomas & Harden, 2008). More than one sentence could make up a code, as well as several codes could be applied to one sentence. For instance, a quote “I’m really torn though, I lead a guild and have [a lot] of friends in-game, but I’d like to quit and live my life” (Carmona & Whiting, 2021) was coded as “Deciding to quit is difficult” and “Social pressure to continue playing”. Each transcript was analysed in turn. Although codes could be used across transcripts, the emphasis during this stage of analysis was on capturing the richness and diversity of data in codes. Line-by-line coding yielded 268 codes. After this all transcripts were reviewed again to a) check the validity of codes, and b) determine if any additional coding was needed. This process resulted in multiple codes being added, removed or amended, bring the final number of codes to 290.
Codes were grouped together based on similarities in meaning. A new label was given to each group, making them into descriptive themes. For instance, “Deciding to quit is difficult”, “Weighing up advantages and disadvantages” and “Decreasing gaming time as a conscious choice” were grouped into “Deciding to quit” descriptive theme. There were 17 descriptive themes. In order to “go beyond” the data to generate new insights and concepts (Thomas & Harden, 2008) the first (KV) and the second (AK) authors, guided by the research question, reviewed descriptive themes in terms of their relevance to the process of recovery from GD. Several themes representing recovery were identified, such as “Process of realization”, “Deciding to quit”, “Social support” and “Quit or reduce playtime”. Through this process it was noted that the unifying characteristic of most studies was that participants went through similar stages on their journey through gaming addiction. Therefore, the analytic themes were developed around these stages, trying to capture key (sometimes different or conflicting) processes of each stage.
Results
Included Studies
The search returned 9,262 records. After sifting by title and abstract, 31 records remained. Excluded records focused on other behavioural addictions, sports, serious games, gaming as a therapeutic tool, exergaming, and quantitative studies on GD. After assessing full-text records, 5 records met the inclusion criteria. Additional 3 records were identified through reference lists of included studies and Google Scholar. In total, 8 studies were included in the review. These studies were marked with an (*) in the list of references. See Figure 1 for PRISMA diagram.
Figure 1. PRISMA Diagram.
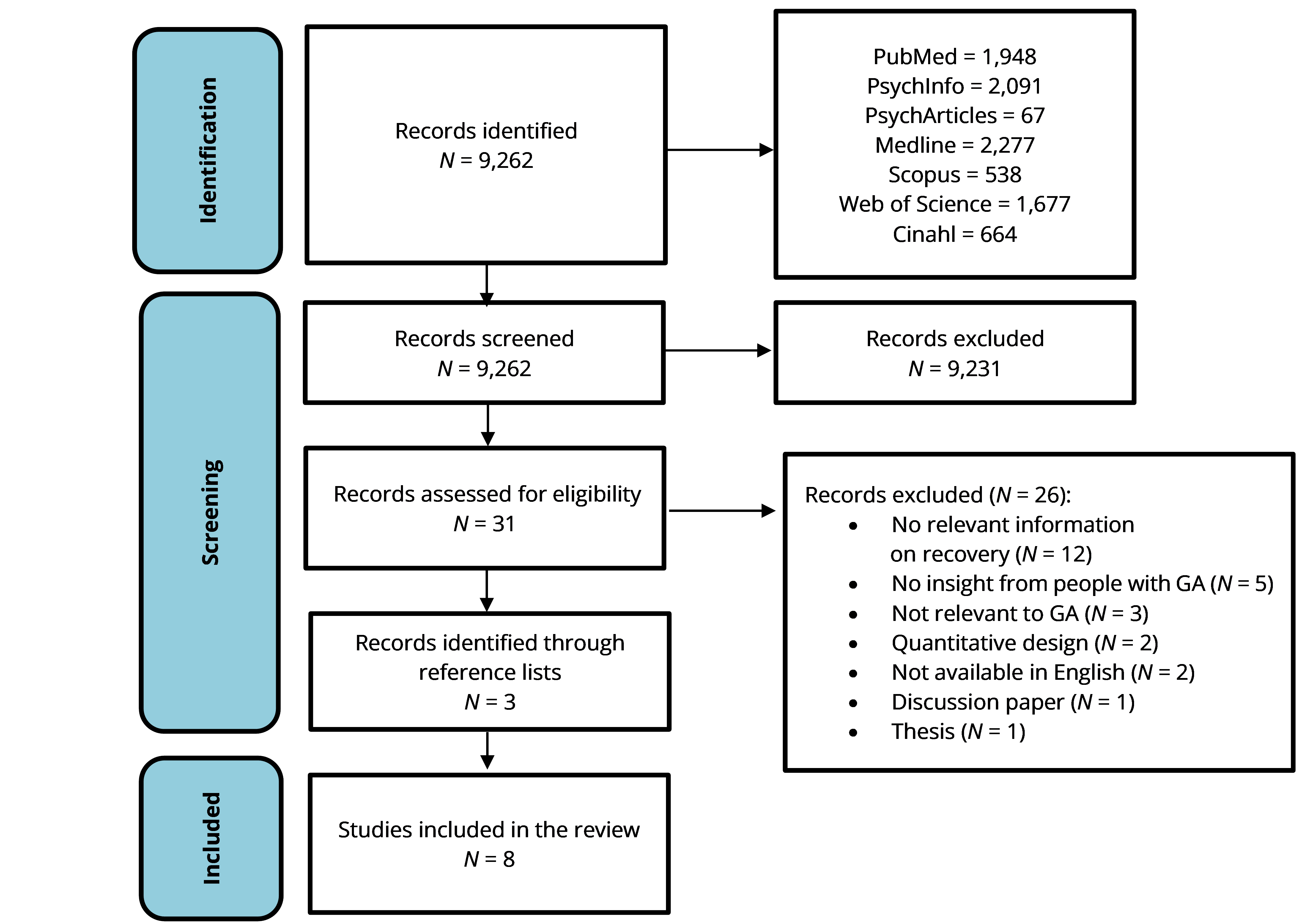
Study characteristics can be found in Table A3. Studies were published in the period between 2006 and 2022. Research was conducted in seven different countries: Spain, Chile, The Netherlands, Finland, New Zealand, Singapore, and Germany. In total, there were 225 participants. The sample was predominantly male (92%). Reported mean age ranged from M = 15.3 (Sim et al., 2021) to M = 30.4 (Karhulahti et al., 2022). Most studies recruited participants who were either undergoing or completed treatment. Participants were recruited through various institutions (hospitals, treatment programs, addiction centres) and in the community (adverts, flyers, posters, snowballing). Two studies obtained data from online forums, so no participant characteristics were obtained (Carmona & Whiting, 2021; Chappell et al., 2006).
All studies employed qualitative methodology. Data was collected through semi-structured interviews or forum posts. Data was analysed using Grounded Theory, Interpretative Phenomenological Analysis, Thematic Analysis or Qualitative Content Analysis. The primary aim of five studies was to understand gaming addiction through a qualitative lens from the perspective of individuals affected by it (Beranuy et al., 2013; Carmona & Whiting, 2021; Chappell et al., 2006; Haagsma et al., 2013; Karhulahti et al., 2022). Two studies evaluated GD treatment programs for adolescents (Sim et al., 2021; Wendt et al., 2021). One study sought to identify optimal components of a health care system for early intervention and treatment of gaming addiction (Park et al., 2021).
Quality Appraisal
Quality appraisal was conducted using the Critical Appraisal Skills Program checklist for qualitative studies (CASP, 2018). The purpose of quality appraisal is to evaluate the rigour of studies included in the review. CASP checklist consists of 10 questions evaluating studies’ methodology, ethical issues and application of findings. Questions are answered either with “yes”, “can’t tell” or “no”. If a question was answered with “yes”, then the criterion was met. If a question was answered with “can’t tell” or “no”, the criterion was not met. CASP guidelines do not provide a scoring system, therefore, studies’ quality was judged by the authors based on the number of met criteria (CASP, 2018). No studies were excluded based on their quality.
Three studies met between 9–10 criteria and were considered of excellent quality (Carmona & Whiting, 2021; Karhulahti et al., 2022; Park et al., 2021). Two studies met between 7–8 criteria and were considered of good quality (Sim et al., 2021; Wendt et al., 2021). Finally, three studies met 6 criteria and were considered of medium quality (Beranuy et al., 2013; Chappell et al., 2006; Haagsma et al., 2013). The best reported elements were whether qualitative methodology was appropriate to answer the research question(s), whether data was collected in a way to answer the research question(s), and whether there was a clear statement of findings; all studies met these criteria. The least reported element was whether the relationship between the researchers and participants was considered; only two studies mentioned it (Carmona & Whiting, 2021; Karhulahti et al., 2022). See Table A2 for full details.
Thematic Synthesis
Articles included limited data on the process of recovery. Only one study had a theme dedicated to recovery (Carmona & Whiting, 2021), and another one had a theme on decreasing gaming time (Haagsma et al., 2013). Other studies discussed recovery in the context of participants’ wider stories of addiction (Beranuy et al., 2013; Chappell et al., 2006; Karhulahti et al., 2022; Park et al., 2021) or in terms of treatment impact (Sim et al., 2021; Wendt et al., 2021). Recovery processes were captured in six themes: “Developing awareness”, “Deciding to change”, “The process of quitting”, “The challenges of quitting”, “Recovery never stops” and “Treatment for gaming addiction”. An overview of themes and subthemes with contributions of each study can be found in Table A4.
Developing Awareness
Developing an understanding that gaming was a problem often appeared as the first step to recovery. For a small number of people, the realization came instantly, like a lightbulb moment: “Then it hit me I had been obsessing over this game in the same fashion for a long time” (Haagsma, 2013). However, the majority described a process of dawning realization, whereby they developed an awareness of their problematic behaviour over time. This was often driven by the negative consequences of excessive gaming, such as loss of relationships, failing at school/university, losing work, deteriorating physical and mental health.
Awareness could also be developed through changing sense of identity or life goals. Individuals realised that their personality has changed because of gaming: “I went from a person who gained energy, pleasure and release from being sociable … to someone who finds it taxing to spend many hours around family and friends” (Carmona & Whiting, 2021). Recognising the destructive impact of gaming on identity drove individuals to re-evaluate their engagement with it: “One day I just started to feel sick, I had to leave and go find myself again … I’ve only now come to understand what [those years] cost me” (Karhulahti et al., 2022). Furthermore, individuals realised that gaming stood in the way of their life aspirations, they would be unable to achieve their goals if they continued playing excessively.
In some cases, awareness was developed when individuals’ relationship with gaming changed. Players realised that despite enjoying gaming initially, at some point it stopped being fun and satisfying:
“I eventually did get burned out and had thoughts of quitting the game entirely... I hadn’t even realized I had been playing in such an obsessive fashion up to that point.” (Haagsma, 2013)
This was supported by a realisation that achievements and skills obtained through gaming were meaningless outside of it. No matter how well individuals performed in gaming, most of the skills and knowledge could not be transferred to real life.
Deciding to Change
Becoming aware of the detrimental impact of gaming led individuals to a shift in perspective to the importance of gaming in their lives, and a subsequent decision to change their behaviour. People used different ways to facilitate this process, e.g., weighing up advantages and disadvantages of playing or re-evaluating their current priorities in life. But in the end, they realised that gaming was an obstacle to whatever they wanted to achieve in real life. Individuals developed a sense that they were missing out on life, realising that other activities were more valuable than gaming: “I can do other things, which is more meaningful than playing computer for the whole day, like reading a book, doing my homework, and having family time” (Sim et al., 2021). Individuals compared virtual and real lives, and the former started losing its attractiveness, consolidating participants’ decision to change their behaviour:
“I have begun to realise how much of a time sink EQ [EverQuest] is. I often think about how having a meaningful romantic relationship just doesn’t fit with EQ dominating my life. For the last few months I have let EQ be my social life, and it’s just recently begun to dawn on me how pathetic it’s become.” (Chappell et al., 2006)
Although many participants did want to fully quit gaming, others wanted to achieve a reduction in gaming time. Individuals who wanted to quit gaming felt that it stopped being a meaningful activity for them, and if they continued, it would only be taking away from their life. They have already lost many valuable things, like time, relationships, or health, so they no longer wanted gaming influencing their lives any further: “[I am] trying to quit, why, [because] this game [has] made me lonely, so god damn lonely that it hurts and I break down crying sometimes” (Carmona & Whiting, 2021). On the other hand, some individuals wanted to continue playing, but change how they engaged with gaming. In Sim et al. (2021) study five out of ten participants chose to reduce gaming time rather than abstain, and in Wendt et al. (2021) study a treatment goal was to teach participants how to control their gaming behaviour, rather than to promote abstinence.
The Process of Quitting
Some individuals were able to quit nearly instantly by crossing gaming out of their lives (Carmona & Whiting et al., 2021; Chappell et al., 2006). There seemed to be very little time passing between an individual deciding to quit and doing it: “I went back to the dorm, said goodbye to my EverQuest friends, and logged off for the last time” (Chappell et al., 2006). Others, by contrast, found it very difficult to cut all ties with gaming, instead going through a process of slowly withdrawing from it: “I have been slowly weaning away but thinking about anything but the game has been hard” (Carmona & Whiting, 2021).
Change was achieved via different ways. Help was sought from hospitals, counselling, addiction recovery centres and specialised programs. Practical strategies for quitting were finding activities to replace gaming, getting rid of gaming accounts and hardware, installing applications blocking access to gaming content, quitting with another person, restrictions set by parents, and taking on real-life responsibilities (Carmona & Whiting, 2021; Haagsma et al., 2013; Karhulahti et al., 2022). Social support was mentioned as an important factor that helped individuals follow through with quitting (Carmona & Whiting, 2021; Karhulahti et al., 2022). Several individuals attributed their successful recovery efforts to receiving support from family, partners or friends: “I am so lucky that my sister loved me enough to save me from myself” (Chappell et al., 2006).
The Challenges of Quitting
Social Ties
One of the key elements that made quitting difficult was the social pull of the game. As many individuals became high-ranking players, they felt that their teammates were relying on them to successfully complete in-game challenges. Hence, there was a deep sense of responsibility, not wanting to let other people down: “I’m really torn though, I lead a guild and have [a lot] of friends in-game, but I’d like to quit and live my life” (Carmona & Whiting, 2021).
Furthermore, individuals forged ties of friendship with other players. When trying to quit, therefore, they often faced pressure from their online friends to come back to the game and play again: “The other day one of my clan told me to connect and play with them. I told them that not yet, maybe later” (Beranuy et al., 2013). One study noted that gaming culture discouraged help-seeking and normalised playing long hours, making individuals feel ashamed of coming out to their online friends about having a “gaming problem” (Park et al., 2021).
However, the forging of strong in-game social ties came at the expense of negative real-life consequences. Gaming provided access to online social communities that were friendly and welcoming, a haven from the outside world. On the flip side, becoming heavily involved with online communities often meant that players withdrew from real-life social interactions. Through the process of quitting some individuals had to face up to their loneliness and a lack of social support in real life. Although some tried to keep in touch with their online friends outside of gaming, this often proved difficult. Gaming was their only common interest, and speaking to these friends rekindled the desire to play:
“A friend just asked me to come and play again, as there was an event that gives a free mount [virtual game item] … I’ve already decided to never play again let alone collect any mounts, and then I hear that I might lose a mount that I’d never ever want, and I will instantly start wanting it and feel disappointed.” (Karhulahti et al., 2022)
An Exciting Activity
Even though it was mentioned in “Developing awareness” that over time gaming stopped being fun, this was not the case for all individuals. Though they spent years playing, some still found gaming to be the most engaging and stimulating activity in their lives. Despite understanding the negative consequences it brought them, there was sadness to having to give up gaming: “When I play, it’s like all the cells in my body scream ‘this is what we were made for!’ It is such a pleasurable, activating and stimulating feeling … and that’s very sad” (Karhulahti et al., 2022). These people recognised that they could not play casually without getting too invested and spiralling into addiction. This made the process of quitting even more difficult, as these individuals felt that they may never encounter an activity that would be as fun and fulfilling as gaming.
An Ingrained Habit
Over the months and years of playing, gaming has become an integral part of peoples’ lives, and their main way of managing and occupying free time. Individuals often resorted to gaming when feeling bored or lonely: “One day, in which you’re home alone, have nothing to do and nobody calls you … I’ve just moved for my basic necessities, take food and that´s all, just play” (Beranuy et al., 2013). Thus, an important element of recovery was to engage in new activities and develop new hobbies to fill the free time left after quitting. However, doing so was often challenging, as individuals found they had reduced motivation and focus, felt controlled by gaming, or no longer had real-life friends to spend time with.
A Way of Coping
People who started playing as a way of escaping the troubles of real life continued to rely on gaming as their main way of dealing with life’s difficulties. Although gaming helped individuals cope, it came at the cost of spiralling into addiction again: “[But] I didn’t even get any interviews, so then one day I went to see a friend with my laptop, started playing again and … that’s a blur for next half a year again” (Karhulahti et al., 2022). Thus, it was difficult to stop gaming in the absence of more adaptive coping mechanisms.
Recovery Never Stops
Coming to Terms With Loss
In some accounts there was a sense that the action of giving up gaming was, in some ways, only the first step to recovery (Carmona & Whiting, 2021; Chappell et al., 2006; Karhulahti et al., 2022). What followed was a long process of rebuilding one’s life anew. Quitting gave individuals space and time to fully acknowledge how gaming has impacted their lives. Often this meant recognising and coming to terms with the negative consequences. Many regretted picking up gaming in the first place, because the impact of addiction was damaging and long-lasting. As an example, a participant in Chappell et al. (2006) study lost his job and family because of the addiction, but even after quitting he could not put things right, as his wife met somebody else, and he rarely saw his children.
Abstinence Is the Only Option
Although some players chose a reduction of gaming time as their recovery goal (Sim et al., 2021; Wendt et al., 2021), others were adamant that complete abstinence from gaming was their only choice (Chappell et al., 2006; Karhulahti et al., 2022). Individuals often framed their decision in biological terms, such as having an “addictive personality” or something being wrong with their brain: “I’ve been trying to tackle other elements around addiction such as alcohol and marijuana, but the truth is I have an addictive personality that extends to many areas of my life” (Park et al., 2021). Such language demonstrates individuals’ conviction that gaming addiction is (at least partly) biologically determined, so they would be unable to control their gaming behaviour if they tried playing casually.
Desire to Continue Playing
Despite recognising the destructive impact of gaming, the desire to play never fully went away. Staying clean from gaming was seen as a constant battle, a difficult choice that individuals had to make every day, prioritising their wellbeing over the thrill of gaming:
“It is so difficult, maybe because I am weak, but even though I consider my life to be successful and happy, there is always EQ, sitting there at the back of my mind, and the desire to play is strong, almost like the pull of the ring in LOTR [Lord of the Rings].” (Chappell et al., 2006)
In addition to these cravings, some people experienced withdrawal-like symptoms. One player mentioned that not having the ability to play made them feel nervous and anxious. When not playing, individuals were preoccupied with thoughts about gaming. The urge to play again could be triggered by talking to friends who still play, watching videos about gaming, visiting gaming-related websites, thinking about how good gaming felt and others.
Relapse
Relapse was mentioned briefly by four studies (Bearnuy et al., 2013; Carmona & Whiting. 2021; Haagsma et al., 2013; Karhulahti et al., 2022). Individuals relapsed after not playing for weeks or even months. Some felt that they could play casually but quickly spiralled into addiction again. Others came back for their social communities, or after being convinced to play again by friends. Relapse could also be triggered by the same factors that started the addiction, e.g., to escape stress or conflict. Several individuals described having an on-off relationship with gaming, stopping for a short while, then coming back to it and playing even more intensely to make up for the progress lost while not playing. Several players mentioned that they came back after a new expansion or update was released.
Being Free From Gaming
One study described the positive impact of recovery (Carmona & Whiting, 2021). The recovery journey was long and difficult for many, so upon finally quitting they felt a great sense of relief and achievement. Individuals described a sense of liberation: they escaped the clutches of gaming and were now free to spend their time on more meaningful activities. People felt excited and hopeful, looking forward to a future without the influence of gaming.
Treatment for Gaming Addiction
Barriers to Treatment-Seeking
Various psychological, social and physical barriers have been cited as reasons for not seeking help for problematic gaming (Park et al., 2021). The addiction itself could dominate a person’s life to such an extent that seeking help became difficult:
“The fact that I did not have the willpower to break away made me feel weak and made me even more depressed! I was on the verge of going to my doctor and asking for some pills, or therapy, or something… but that would break into my WoW-time!” (Carmona & Whiting, 2021)
Individuals reported feeling a deep sense of shame and embarrassment at admitting that they had a “gaming problem”. They felt that gaming was a “soft addiction”, not as severe as substance misuse or other mental health issues. This view was reinforced by perceived negative social attitudes and stigma towards problematic gaming.
Many practical barriers were reported, such as a lack of knowledge/availability of services; the cost of paying for services; services perceived to be geared towards treating adolescents, rather than adults, and others. Some individuals who tried accessing support felt that services did not understand what GD was and how to treat it. Lack of services reinforced the idea that problematic gaming was not a problem worthy of treatment.
Helpful Treatment Components
Two studies (Sim et al., 2021; Wendt et al., 2021) explored adolescents’ experiences with group treatment for gaming addiction. Participants thought that it was important for therapists to be understanding, non-judgemental and trustworthy. In Sim et al. (2021) study therapists acted as role models, for instance, showing how to play games in a healthy way by regulating gaming time during therapeutic group gaming sessions. Regarding treatment elements, participants found the following useful: psychoeducation, understanding the roots of problematic gaming, exploring individual problems, time management, developing a daily plan, and having individual therapy sessions. Most participants were in favour of the group setting of therapy, as it encouraged participants to build real-life social connections and support each other on their recovery journey. Furthermore, when someone successfully achieved a goal, it motivated others to work harder. Participants engaged with treatment better if they were allowed to have fun in sessions, play together and engage in other activities, such as outdoors games.
Unhelpful Treatment Components
The unhelpful treatment components primarily concerned group composition and dynamics (Sim et al., 2021; Wendt et al., 2021). Treatment group in Wendt et al. (2021) study had mixed group composition (in-patient and community) which participants found difficult to adjust to. Some individuals found it challenging to be open in front of other group members due to being shy or having social anxiety. There was also a concern that therapists did not equally allocate time to every person, instead focusing on two or three individuals each session. Some participants were dissatisfied if modules covered in treatment were not personally relevant.
Positive Impact of Treatment
Individuals reported that treatment was helpful in a range of ways, for instance, it improved their insight and made them feel more mature (Sim et al., 2021; Wendt et al., 2021). Treatment helped participants to develop skills for controlling their gaming behaviour (such as time management), and, as a result, reduced gaming time. It improved family relations and academic performance. Group composition gave participants an opportunity to create real-life friendships and learn new skills through activities.
Discussion
The purpose of this review was to understand how individuals addicted to video games experience recovery. Of eight studies included in the review, only two discussed recovery in a separate subtheme (Carmona & Whiting, 2021; Haagsma et al., 2013), showing that this concept has been under-explored in qualitative research. The core finding of the review is that individuals go through five processes on the road to recovery from gaming addiction: develop awareness of the problem, make a decision to change their behaviour, employ change strategies, address setbacks and difficulties, and work on sustaining recovery.
Even though these processes could be found across studies, there was significant variation in how participants experienced them. Awareness of gaming being a problem could come like a lightbulb moment or develop gradually over time. A decision to change could be motivated by positive aspirations (wanting to get a new relationship, complete a degree) or negative consequences (failing at school, relationship breakdown). Individuals differed based on whether they wanted to quit gaming and abstain from it in the future or reduce play time and maintain a healthy level of engagement. Finally, when it came to quitting, some individuals were able to quit instantly (i.e., decided to quit and did it straight away), whereas for others it was a long and drawn-out process. Thus, though unified by the same processes, there was significant diversity to how recovery from gaming addiction was experienced.
Reiterating the definition given in the introduction, recovery is a “process of behavior change characterized by improvements in biopsychosocial functioning and purpose in life” (Witkiewitz et al., 2020, p. 9). This definition can be applied to the concept of recovery developed in this review. Individuals sought to change their gaming behaviour by using various strategies (e.g., seeking treatment, selling gaming accounts/hardware), and their life improved as a result. The benefits of overcoming gaming addiction were improved relationships, better academic performance, improved self-awareness, and others. Although the definition implies that a shift in individuals’ purpose in life accompanies behaviour change, current findings suggest that it happens prior to change occurring. After acknowledging that gaming has had a negative impact on their lives, participants re-evaluated their life priorities and aspirations which often led to a realisation that gaming was an obstacle to achieving meaningful things in life, and this became motivation for behaviour change.
Recovery processes identified in this review appear to align with the stages of change proposed by the Transtheoretical Model (TTM; Prochaska et al., 1992). The model has been used extensively to study recovery in other addiction fields and to inform practice (Ferreira et al., 2015; Kushnir et al., 2016; Tseng et al., 2022), meaning that this conceptual framework can also be adapted to gaming addiction and to the present findings. The model holds that every individual goes through five stages while trying to change their behaviour: precontemplation, contemplation, preparation, action, and maintenance (see Table 1). Progression between stages is facilitated by 10 change processes that represent a shift in individuals’ thinking, behaviour or affect. For instance, moving from “precontemplation” to “contemplation” stage is facilitated by a process of consciousness-raising as individuals become aware of the causes, consequences, and cures of their problems (Prochaska & DiClemente, 2005, p. 150).
“Precontemplation” stage was not identified in this study, as most studies included participants who were in recovery or undergoing treatment, indicating that they were already at later stages of change. Theme “Developing awareness” represents the “contemplation” stage when individuals realised that their gaming was problematic. “Deciding to change” was also assigned to “contemplation” stage, as it encompasses individuals thinking about overcoming their addiction, weighing up advantages and disadvantages of doing so. Unfortunately, with the available data, it was not possible to determine whether a decision to change may have also represented an active intention to change behaviour, otherwise this theme would have been assigned to “preparation” stage. Themes “The process of quitting” and “The challenges of quitting” represent the “action” stage of the model. Individuals actively attempted to change their behaviour to overcome the addiction, and encountered various difficulties while doing so, such as struggling to let go of online friendships, finding activities to replace gaming, or developing new coping strategies. Finally, “Recovery never stops” is about “maintenance”, continuing to engage in new behaviours, coming to terms with loss, battling old habits, and managing the desire to play and relapse.
Table 1. Stages of Change and Current Themes.
|
Stage |
Stage description |
Themes |
|
Pre-contemplation |
Individual has no intention to change the behaviour in the foreseeable future. |
|
|
Contemplation |
Individual is aware of the problem and is thinking about overcoming it. |
“Developing awareness” “Deciding to change” |
|
Preparation |
Individual is intending to take action in the near future. |
|
|
Action |
Individual modifies their behaviour or environment to overcome their problem. |
“The process of quitting” “The challenges of quitting” |
|
Maintenance |
Individual works on preventing relapse and consolidating the gains attained during action. |
“Recovery never stops” |
|
Note. Stage descriptions taken from Prochaska et al. (1992). |
||
TTM conceptualises change as a spiral, arguing that achieving long-lasting “maintenance” may require multiple attempts and relapses, it is an iterative process (Prochaska et al., 1992). The present findings support this notion with participants describing episodes of relapse, as well as encountering various challenges that hindered their progression through the stages. Even though studies in the current review tended to mention relapse briefly, research shows that relapse is a core element of addiction recovery, it allows individuals to develop greater awareness of their problematic behaviour and learn better coping strategies (Kougiali et al., 2017).
However, present findings also differ from the TTM conceptualisation of change. Beyond the spiral of relapse, progression through stages is sequential and linear within the model (Prochaska et al., 1992). However, in line with the model’s criticisms (Sussman et al., 2022), current findings indicate that individuals may not necessarily progress through all five stages on their road to recovery. For instance, it could be argued that individuals who quit gaming instantly upon realising it was problematic have gone straight from “contemplation” to “action” stage, missing the “preparation” stage. Similarly, although TTM argues that developing awareness of one’s problematic behaviour is crucial for recovery (Prochaska et al., 1992), other researchers have argued that insight may not be necessary for change to occur (Sussman et al., 2022; White, 2007). Supporting this notion, treatment evaluation studies in this review (Sim et al., 2021; Wendt et al., 2021) contributed limited data to “Developing awareness” theme, indicating that insight may not be necessary to engage in gaming addiction treatment.
While TTM focuses on internal motivation for change, this review found that individuals’ social environments could have a significant impact on the course of recovery. For instance, being part of an online social community and/or not having real-life friends could make it difficult to quit. Previous research has established that removing distractions and creating a secure environment (i.e., going into residential treatment or taking time off work) was important for stability during the initial stages of recovery (Martinelli et al., 2023). Another study found that supportive relationships and mutual aid communities are key to successful recovery (Goshorn et al., 2023). Many individuals in this review felt that social support received from family and friends was imperative for successful recovery.
In line with previous research (Watkins et al., 2021), current review found that identity transformation played an important role in the process of recovery. Addiction “spoils” identities, and recovery involves “identity reverting” (re-engaging in roles and responsibilities individuals had prior to addiction), as well as establishing new roles (developing relationships, gaining employment and education; Reith & Dobbie, 2012). Changing identity from a substance “user” to “non-user” not only allows individuals to think and feel differently about themselves, but also gives a qualitatively different way of relating to others (Martinelli et al., 2023). Present findings similarly indicate that recovery from gaming addiction involves transformation of identity. For instance, over the course of recovery some individuals developed a belief that they were biologically susceptible to addiction. This had implications for self-perception (i.e., their sense of agency, control over gaming behaviour), how individuals made sense of their experiences, and recovery behaviours (i.e., choosing abstinence over reduced play time to stay well). Although the process of identity transformation is considered to be occurring organically in the course of recovery (Watkins et al., 2021), current findings suggest that participants may also consciously engage in it. At the stage of “Developing awareness” individuals actively considered the negative impact of excessive gaming on their identity compared to how they were like before becoming addicted (e.g., becoming reclusive, losing social skills). This realisation caused a dissatisfaction with the present state of self which contributed to individuals’ desire to change their behaviour.
The process of recovery from gaming addiction is comparable to recovery from gambling addiction. Recognition that gambling is problematic comes over time as the negative consequences become more severe (Stefani, 2023), and developing insight is a prerequisite for recovery (Pickering et al., 2020). Identity transformation plays a central role in gambling recovery, with many participants talking about having an “authentic” self and a “gambling” self that are in conflict with each other (Pickering et al., 2020; Reith & Dobbie, 2012; Stefani, 2023). The behaviour of the “gambling” self is perceived as incongruous with people’s values and aspirations which facilitates the process of change (Pickering et al., 2020; Reith & Dobbie, 2012; Stefani, 2023). Similarly to the current study, participants in recovery from gambling underline the significance of having supportive social networks (Nilsson et al., 2023; Pickering et al., 2020).
The question of whether gaming should be studied separately to other Internet-based addictions was raised earlier in the paper. While there is a lot of overlap in how gambling and gaming addictions are experienced, there are also clear differences. This review found that in-game social connections played an important role in the maintenance of gaming addiction. By contrast, engaging with gambling online communities appears to be a protective factor against excessive play (Sirola et al., 2021). Also notably, money plays a crucial role in gambling addiction, but it has not been identified as an issue in the current study. Among participants with gambling addiction many recovery goals are tied to gaining financial stability, employment, and paying off loans (Oakes et al., 2019; Pickering et al., 2020; Reith & Dobbie, 2012). Therefore, it can be seen that the process of recovery from gaming addiction shares similarities with recovery from gambling, but there also unique features.
There were several recovery processes mentioned by the gambling studies that have not been identified by the current study. Participants in Pickering et al. (2020) study spoke about the daily struggles of recovery, such as managing gambling triggers, urges and cravings. Relapse also plays a much bigger role, being a source of significant anxiety, it instilled feelings of hopelessness around the possibility of change (Nilsson et al., 2023; Pickering et al., 2020). Erroneous cognitions and thinking biases were shown to interfere with gambling recovery (Oakes et al., 2019; Pickering et al., 2020). These experiences may be relevant to gaming addiction too, but further research is needed in this area.
Practice Implications
A unique finding of this review was that that individuals’ recovery efforts could be compromised by online friendships, social isolation, a feeling of boredom, a lack of daily structure and other activities/hobbies, and poor coping mechanisms. To address these complexities, treatment interventions must adopt a multidimensional approach. A comprehensive service should offer individuals access to reliable information on GD, validated screening tools, evidence-based treatments, peer support networks, and assistance for co-occurring issues (Park et al., 2021).
Recognizing boredom as a significant barrier to recovery, it is advisable to establish non-gaming activity groups for patients. Furthermore, given that boredom is an obstacle to recovery, it would be useful to organise non-gaming activity groups for patients. There groups would give individuals opportunities to expand their real-life social networks and develop hobbies outside of gaming. In addition, it may also be helpful to introduce pre- and post-treatment support. The review found that some individuals may struggle with insight into their problematic behaviour and may feel ambivalent about change. Research shows that having strong internal, but not external, motivation to change increases the likelihood of being further along the TTM change continuum and feeling more ready to change (Kushnir et al., 2016). Thus, a pre-treatment intervention could provide psychoeducation and screening to raise clients’ self-awareness and foster their internal motivation to engage in treatment. Post-treatment support could provide help around adjustment to life without the addiction, managing cravings to play and relapse. A multi-stage treatment model like this one could address the needs of clients at different points in their recovery journey.
Theme “Recovery never stops” demonstrates that even after individuals quit or improve their gaming behaviour, their recovery continues in the form of coming to terms with loss, managing withdrawal symptoms, cravings to play and relapse. A gambling addiction follow-up study showed that 43.7% of patients relapsed at least once, the average time of a relapse occurring was 1.39 years after first observed recovery (Grall-Bronnec et al., 2021). However, a recent review of the efficacy of cognitive-behavioural therapy for gaming addiction found that follow-ups were conducted 8 weeks to 6 months after treatment (Stevens et al., 2019) which in light of the previous findings may be insufficient to detect relapse and long-term impact of treatment. Therefore, it is suggested that treatments ought to incorporate relapse prevention strategies, and follow-ups should be conducted at longer time-periods.
Limitations and Future Directions
There were several limitations to the current study. The first limitation was that this review was carried out and written primarily by the first author which could have introduced bias into the review process. The second author was involved as the supervisor of the project and provided support around refining superordinate themes and preparing the manuscript. To minimise risk of bias, the first author kept a reflective diary throughout the study, and both authors held regular meetings to discuss how the review process was going.
The second limitation was that the majority (92%) of participants were male. A meta-analysis by Stevens et al. (2021) established that GD male to female prevalence ratio is 2.5:1. None of the studies in this review met this participant ratio, and three studies had male-only samples (Beranuy et al., 2013; Haagsma et al., 2013; Sim et al., 2021). There are sex differences in how GD is experienced, for instance, male gamers score higher on impulsivity and aggression scales, whereas female gamers score higher on depression and social phobia scales (Marraudino et al., 2022). Therefore, it has been suggested that GD treatment should target executive functioning in men and emotional distress in women (Dong & Potenza, 2022). However, further research is needed to test these assumptions and develop better understanding of how recovery processes may vary for men and women.
The third limitation was that the majority of included studies did not discuss recovery directly. Instead, information relevant to recovery had to be inferred from participants’ narratives of addiction. The implications of this for current findings are that, firstly, potentially relevant recovery processes or experiences may not had been mentioned, and secondly, given limited amount of available data, the importance of certain elements could have been over- or under- emphasised. To illustrate, many participants in included studies chose to quit gaming which could give the impression that abstinence is the preferred recovery goal. However, GD treatment studies measure recovery in terms of symptom reduction (Gavriel-Fried et al., 2023) which aligns more with reduced play time recovery goal, rather than abstinence. A gambling addiction treatment follow-up study found that out of 70% of participants who no longer met the criteria for a gambling disorder, 40% abstained and 30% continued to gamble without adverse consequences (Müller et al., 2017). Therefore, it would be useful to explore how the experiences of people who chose reduced play time versus quitting recovery goals may be different. For instance, it is unclear whether experiences identified in themes “The process of quitting” and “The challenges of quitting” would still apply to those who chose reduced play time recovery route.
Although all studies included in the review recruited participants who had some form of addiction treatment, it is unclear what role treatment plays in recovery. “Treatment for gaming addiction” theme outlines the benefits of intervention programs for gaming addiction. However, it is well-known in other addiction fields that people can recover naturally, without ever seeking professional support (el-Guebaly, 2012). Understanding the role of treatment in recovery would allow us to develop more effective ways of supporting individuals battling gaming addiction.
Conclusions
This review offered unique insights into the recovery process from gaming addiction by highlighting that individuals with gaming addiction go through similar processes on their recovery journey: develop awareness of the problem, decide to change their behaviour, employ change strategies, address challenges and setbacks, and work on maintaining recovery after getting better. However, it was also discovered that there is significant variation in how each process is experienced, for instance, whether an individual decides to quit or reduce their play time. Recovery processes identified in this review support previous findings on the role of TTM, social support and identity change in addiction recovery. Nevertheless, further research would be needed to expand our understanding of recovery from gaming addiction, such as about the role of gender differences or the impact of treatment in recovery. Current findings have implications for treatment of gaming addiction, highlighting the importance of a multidimensional treatment approach to address comorbid conditions and co-occurring problems, as well the potential benefits of introducing pre- and post-treatment support.
Conflict of Interest
The authors have no conflict of interests to declare.
Acknowledgement
The literature review protocol was registered with PROSPERO (CRD42022302202).
Appendix
Table A1. SPIDER Framework.
|
Sample |
any |
|
Phenomenon of Interest |
(game* OR gaming) AND (disorder OR addict* OR problem* OR pathology* OR excessive OR overuse OR abuse OR compulsive) |
|
Design |
question* OR survey* OR interview* OR focus group OR case stud* OR observ* OR forum |
|
Evaluation |
view* OR experience* OR opinion* OR attitude OR perce* OR belie* OR feel* OR understand* OR thought* |
|
Research type |
qualitative |
|
Note. SPIDER is a search strategy tool for qualitative literature reviews (Cooke et al., 2012). |
|
Table A2. Quality Appraisal—CASP Qualitative Checklist.
|
Questions/studies |
Beranuy et al. (2013) |
Carmona & Whiting (2021) |
Chappell et al. (2006) |
Haagsma et al. (2013) |
Karhulahti et al. (2022) |
Park et al. (2021) |
Sim et al. (2021) |
Wendt et al. (2021) |
|
1. Was there a clear statement of the aims of the research? |
Yes |
Yes |
Yes |
Can’t tell |
Yes |
Yes |
Yes |
Yes |
|
2. Is a qualitative methodology appropriate? |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
|
3. Was the research design appropriate to address the aims of the research? |
Can’t tell |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
|
4. Was the recruitment strategy appropriate to the aims of the research? |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Can’t tell |
|
5. Was the data collected in a way that addressed the research issue? |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
|
6. Has the relationship between researcher and participants been adequately considered? |
No |
Yes |
No |
No |
Yes |
No |
No |
No |
|
7. Have ethical issues been taken into consideration? |
Yes |
Yes |
No |
Can’t tell |
Yes |
Yes |
Yes |
Yes |
|
8. Was the data analysis sufficiently rigorous? |
Can’t tell |
Yes |
Can’t tell |
Can’t tell |
Yes |
Yes |
Can’t tell |
Can’t tell |
|
9. Is there a clear statement of findings? |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
Yes |
|
10. How valuable is the research? |
No |
Yes |
Can’t tell |
Yes |
Yes |
Yes |
Yes |
Yes |
|
Note. CASP Qualitative Checklist is a quality appraisal tool used to assess the rigour of qualitative papers included in literature reviews. Questions are split into three sections assessing validity (questions 1–6), results (questions 7–9) and applicability of findings (question 10). A criterion was met if a question was answered as “yes”, and unmet if answered as “no” or “can’t tell”. Study quality was categorised as excellent (9–10), good (7–8) and medium (6). |
||||||||
Table A3. Data Extraction.
|
|
Location |
Study aims/questions |
Context |
Recruitment |
Methodology |
N* |
M, range* |
Nf* |
Data collection |
Data analysis |
Was any data excluded from analysis?*** |
|
Beranuy et al. (2013) |
Spain Chile |
1. Understand problematic gaming and its function. 2. Compare symptoms and consequences to more established addictions. |
Participants sought treatment from hospitals for excessive gaming. In all but one case treatment was instigated by the mother. Participants were either undergoing or completed treatment, however, it was not specified what treatment they received. |
Hospitals |
Grounded Theory |
9 |
20.50 |
0 |
Semi-structured interviews |
Grounded Theory via Atlas.ti |
No |
|
Carmona & Whiting (2021) |
N/A |
1. How do self-described WoW addicts describe their development of addiction? 2. How do these gamers’ descriptions reflect how the DSM codifies addiction phenomena? 3. How do gamers describe their efforts to recover from addictive behaviours? |
Data was obtained from two websites dedicated to sharing addiction and recovery stories from World of Warcraft (wowdetox.com & reddit.com/noWoW). Posts ranged from 100 to 1,800 words in length and were posted in the period between 2006 and 2011. |
N/A |
Grounded Theory |
140 |
12+** |
14** |
Forum posts |
Grounded Theory |
No |
|
Chappell et al. (2006) |
N/A |
To examine how individuals perceived and made sense of EverQuest in the context of their lives. |
Data was obtained from various forums where participants discussed their experiences of being addicted to EverQuest. Participants were at different stages of recovery: relapse, still actively playing or quit. |
N/A |
Phenomeno-logy |
12 |
N/A |
N/A |
Forum posts |
Interpreta-tive Phenome-nological Analysis |
No |
|
Haagsma et al. (2013) |
Netherlands |
To contribute to a more dynamic understanding of the complexity of excessive gaming in general and the way in which changes in cognitions interact with behavioural trajectories in particular. |
Participants were recruited if they were experiencing or had experienced problems related to gaming. Participants differed based on their age, occupation (secondary school, vocational school, university, working), and time spent gaming (few hours to 66h currently, 10h to 105h historically). |
Flyers, adverts, emails, addiction centre, snowball |
Qualitative |
21 |
N/A |
0 |
Semi-structured interviews (face-to-face) |
Thematic Analysis |
No |
|
Karhulahti et al. (2022) |
Finland |
To explore the differences and similarities between gamers who are seeking treatment (potential GD) and e-sports gamers (no self-reported problems). |
Adult working population, students were excluded. Participants were not screened, but it was assumed that their presentation was sufficiently severe, since they sought treatment. Participants’ treatment stage differed from recovery to still affected by disordered gaming. |
Hospitals, therapy centres, medical institutions |
Phenomeno-logy |
6 |
30.40 |
1 |
Semi-structured interviews (video using Pheno-menology of Play protocol) |
Interpreta-tive Phenome-nological Analysis via Atlas.ti |
Yes (Data from esports gamers and experts was excluded—themes “Esports players: i), ii), iii)” and “Meanings by experts”) |
|
Park et al. (2021) |
New Zealand |
1. Describe the experiences and needs of people seeking help for gaming problems. 2. Identify the optimal components of a health care system to support early intervention and treatment of gaming problems. |
Participants were recruited from a larger study examining the impact of a brief online intervention for gaming problems. This larger study involved 50 gamers who wanted to limit or reduce their gaming within 30 days. Participants had to be 18 or older and not currently seeking in-person treatment. |
Social media adverts, posters, snowball |
Person-centred access to health care framework |
20 |
23.00 (20–35) |
2 |
Semi-structured interviews (instant messaging) |
Qualitative content analysis via Nvivo |
No |
|
Sim et al. (2021) |
Singapore |
1. What are the adolescents’ and their parents’ views on and experiences of the different treatment components of the CWEP? 2. What are the adolescents’ and their parents’ views on and experiences of some of the unique mechanisms of the CWEP? |
Evaluation of Cyber Wellness Enrichment Program for treatment of problematic gaming. It includes four main components: 1. Individual counselling (managing time & gaming habits), 2. Family counselling, 3. Group mentoring & social support, 4. Alternative activities. Treatment emphasises healthy engagement with games, rather than abstinence. The length of the program is 3 months. |
Cyber Wellness Enrichment Programme |
Qualitative |
10 |
15.30 |
0 |
Semi-structured interviews |
Qualitative content analysis via Nvivo |
Yes (Parents’ perspectives were excluded) |
|
Wendt et al. (2021) |
Germany |
To conduct a qualitative investigation of young IGD patients and clinical experts to contribute to a better understanding of treatment requirements for this disorder. |
Treatment was administered at the inpatient and day-clinic service for adolescents with substance and behavioural addictions. The GD group intervention consisted of 8 modules, each session 60 minutes long. Treatment included psychoeducation, control strategies, understanding relationships and others. This intervention was part of the service treatment offer that also included individual therapy, medication, occupational and sports therapy, family support and others. |
Day clinic, ward for addictions |
Qualitative |
7 |
15.86 |
1 |
Semi-structured interviews |
Qualitative content analysis via MAXQDA |
Yes (Data from experts—theme “3.2 Interviews with Experts”) |
|
Note. Data extraction for every study included in the review is given in this table. *Participant characteristics (N, M, range, Nf) are given for participants whose data was included in the analysis, e.g., Sim et al. (2021) had a sample of adolescents and a sample of parents, but only adolescents’ characteristics were included. **This data was an estimation, given that forum posts were anonymous and did not always include person’s age and gender. ***The primary goal of this study was to explore the process of GD recovery from the perspective of people affected by it. Therefore, themes discussing the experiences of other people (affected others, healthy gamers, experts) were excluded from the analysis. |
|||||||||||

This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Copyright © 2024 Ksenija Vasiljeva, Alex Kyriakopoulos, Christopher Wilson